

>Pharmacodynamics deals with the biochemical and physiological effect of drug as well as its mechanism of action.
OR
We can simply define it as, The action of drug on the body.
•Most drug exert effects, both beneficial and harmful, by interacting with specialized target macromollecule called receptor.

Receptor : it refers to the drug binding site in the cell or on the surface of cell which mediate the action of drug.
• There are some drugs which do not require receptors Example = mannitol , anti-helmintic drugs, etc.
NATURE OF DRUG RECEPTOR
1. Regulatory protein which mediates the action of endogenous chemical signals. For example : neurotransmitters , harmones and autocoids.
2. Enzymes. For example : dihydrofolic reductase
3. Transport protein. For example : sodium / potassium ATPase pump.
4. Structural protein. For example : tubulin.
RECEPTOR REGULATION
•Down Regulation : when receptors become desensitized or decrease in number when exposed to agonist repeatedly.
•UP Regulation : when receptors supersensitive to agonist via synthesis of additional receptors on chronic administration of antagonist.
SPARE RECEPTORS
• When maximal response can be elicited by an agonist at the concentration that does not result in occupancy of all available receptors, the receptors that are not occupied are called spare receptors.
OR
We can simply define it as more(extra) receptor available than needed to elicit the maximum response.
=>When drug binds with receptor, it form drug receptor complex, Which initiated alterations in biochemical or mollecular activity of a cell by process called Signal transduction.

SIGNAL TRANSDUCTION
Drug act as signals, and receptors act as signal detectors. A drug is termed as “agonist” if its binds to a site on receptor protein and activated it to initiates a series of reactions that ultimately result in specific intracellular response.
• “2nd messenger” or effector mollecules are part of cascade of events that translate agonist binding in to cellular response.
1. The Drug Receptor complex
• Cells have many different types of receptors each of which is specific for a particular agonist and produce a unique response. For example : cardiac cell membranes contain ‘B-adrenergic receptors that binds and response to epinephrine or norepinephrine. Cardiac cells also contain muscarinic receptors that binds and response to acetylcholine.
These 2 receptors population control heart vital functions.

=>The magnitude of the cellular response is proportional to the number of drug-receptor complexes. More the D-R complex more will be response.
When drug binds with recptors, it produce a measurable response via :
2. Major receptor families
• A receptor is defined as any biological mollecule to which drug binds and produce response. Ghus enzymes, nucleic acids & structural proteins can act as receptors for drug or endogenous agonists. How ever richest source of receptors are membrane bound proteins. There are following types of receptors :
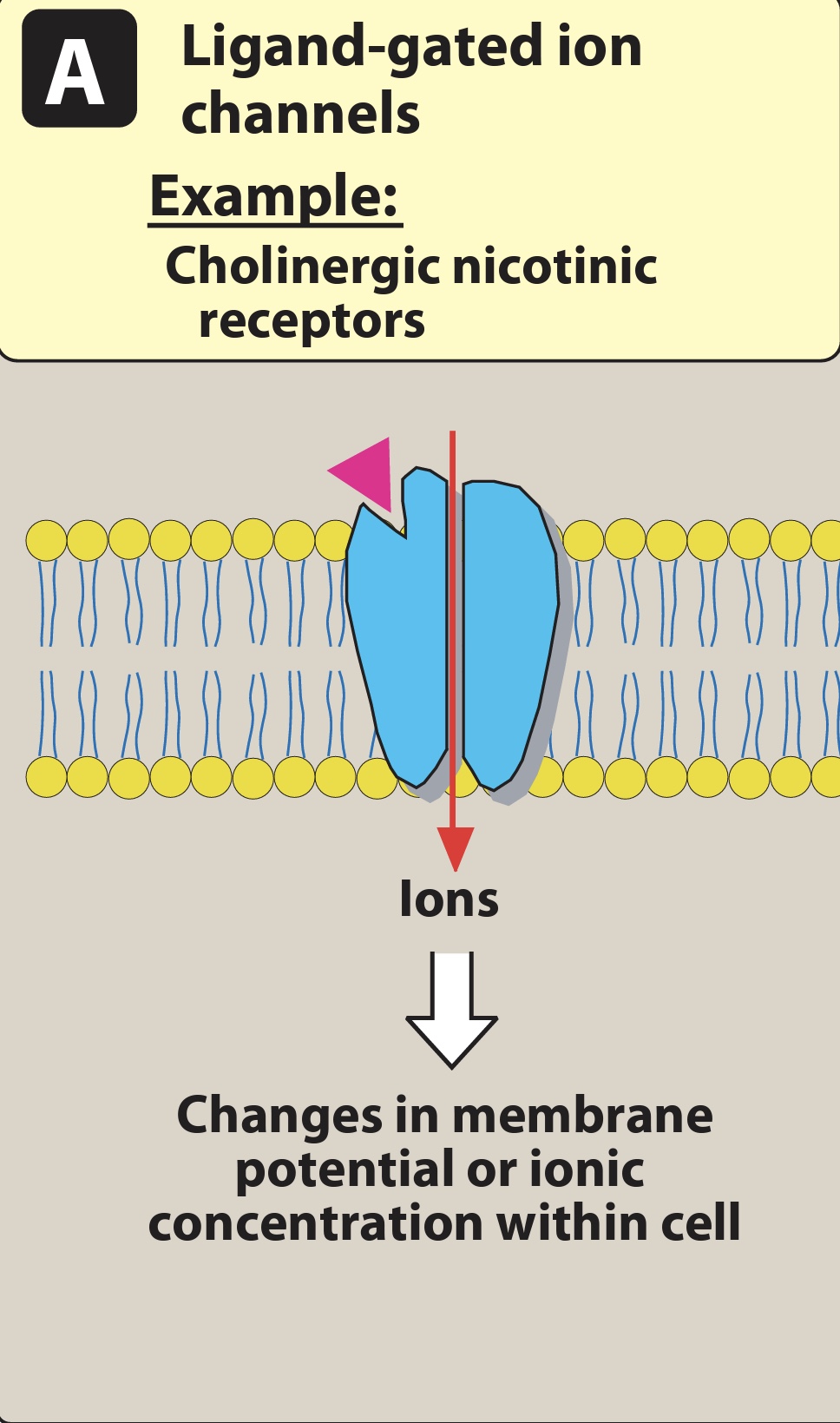
(i) Cell membrane receptors coupled to ion/ligand gated channels
• The extracellular portion of ligand gated ion channels contains drug-binding site. The site regulated the opening of pore through which ions can flow across cell membranes. The channel us usually closed untill the receptor is activated by an agonist, which open the channel for few milli seconds.
For Example : acetylcholine stimulated the nicotinic receptors that cause the channels to open, that allows Na influx and K outflux across the C.M(cell membrane) of nuerons or muscle cells. The change in ionic concentration across C.M generated an action potential in neuron and contraction in skeletal and cardiac muscles.
On the other hand GABA receptor increase the Chlorine influx, resulting in hyperpolarization of neurons and less chance of generating action potential.
Another example is Local anesthetics : these will bind with voltage gated Na channels, inhibiting the Na influx and decreasing the neuronal conduction.
(ii) Transmembrane G- protein-coupled receptors:
• The extracellular portion of this receptor contains the ligand-binding site and the intracellulular portion interacts(when activated) wit G protein.
G proteins are of many kinds ( Gs, Gi, Gq) but all these types are composed of 3 protein subunits. The alpha subunit binds with GTP and Beta & gamma subunits binds anchor the G protein in the cell membrane.
— Gs => stimulates the adenyl cyclase that cause the conversion of ATP to cAMP then cAMP activates protein kinase A which on further promotes phosphorylation of protein (tissue specific enzyme) activation.
Example : Histamine(H2) and serotonin(5HT) receptors.
—Gi => It inhibits the adenyl cyclase that will cause inhibition of cAMP production.
Example : sympthatic(alpha 2) and muscarinic(M2) receptors.
—Gq => It activates phospholipase C which increase the IP3 production that cause Calcium release from sarcoplasmic reticulum. Ca++ activates the protein kinase C that cause the phosphorylation of proteins.
Example : aplha1, M1, M3, angiontensin (AG11) , & opiod receptors. 


(iii) Intracellular receptors :
• This family of receptors differs comsiderably from others in that the receptor is entirely intracellular. Therefore ligand must have lipid solubility to diffuse in to cell to interact with receptors.
—- when lipid soluble ligand enter in Cell it form harmone-receptor complex, which will cause stimulation of response elements on DNA that modifies gene expression( formation of mRNA from DNA and translate information of mRNA to make proteins)

Othe targets of intracellular ligands are structural proteins, enzymes, RNA, ribosomes.
• They have slow onset but long duration of action.
Comments